1701006039 - long case
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
A 60year old female came to the opd with the
CHIEF COMPLIANT:
cough with sputum since 10days
breathlessness since 10days
HOPI:
patient was apparently asymptomatic 10days back
Then she has developed cough with expectoration which is insidious in onset, gradually progressive and associated with whitish colour, mucoid,non foul smelling,non blood stained
Aggravates on lying on left side and during night times
Breathless of grade 2 mmrc(i.e walk slower than other people of same age due to shortness of breath) since 10days
Which is associated with wheeze
H/o low grade fever with chills and rigor which is on and off since 10days which relieved by medications
H/o of weight loss, burning micturation
No h/o night sweats(r/o tb)
No h/o orthopnea,pnd ,chest pain , palpitations
No h/o lower limb swelling, reduced urine output, change in voice
No h/o seasonal variation of above symptoms
PAST HISTORY:
h/o similar complaints in the past 5year back which relieved by medications
H/o diabetes mellitus past 6year on medication (metformin)
No h/o tb,asthma,htn, epilepsy, thyroid
PERSONAL HISTORY
diet-mixed diet
Appetite -normal
Sleep -adequate
No addiction
Bowel and bladder -regular:
GENERAL EXAMINATION
patient was conscious, cooperative and oriented to time,place and person
Well nourished and moderately built
No pallor
No icterus
No cyanosis
No clubbing
No pedal edema
No lymphadenopathy



External marker of tb-choroid tubercles,phlycten,scars/sinuses,cold abscess/collar stud abscess absent
No external marker of malignancy
Vitals-
Temperature -99°F
Pulse rate -100/min
Respiratory rate -22/min
Bp-120/80 mm Hg
Spo2-97%
Grbs -307 mg%
Respiratory system examination:
Upper respiratory tract:
Nostrils -normal
No Dns,nasal polyps,sinus tenderness
Oral cavity -normal
Oral hygiene is maintained
No dental caries
Posterior pharyngeal wall - normal
LRT:
Inspection:
Shape of chest- normal(bl symmetrical , elliptical)
Spine normal
Trachea appear to be central
Chest movement equal on both sides
Pattern of breathing thoraco abdominal
No usage of accessory muscles
No dropping of shoulder
Skin over the chest normal
No scars ,sinuses ,visible pulsation
Palpation:
All inspectory finding are confirmed
Spine normal
Trachea central
Apex beat palpable at 5th intercoastal space ,1cm medial to mid clavicular line
No local rise of temperature
No tenderness
Dimensions of measurement
Transverse diameter -12inches
Anterior posterior diameter -10.5inches
Td:ap diameter -1.14
Chest circumference -87cms
Percussion
Areas. Right. Left
Supraclavicular resonant Resonant
Clavicular resonant Resonant
Infraclavicular resonant Resonant
Mammary resonant Resonant
Axillary resonant Resonant
Infraaxillary resonant Resonant
Suprascapular resonant Resonant
Interscapular resonant Resonant
Infrascapular resonant Resonant
AUSCULTATION
Areas. Right. Left
Supraclavicular normal normal
Infraclavicular normal normal
Mammary. Normal. Normal
Axillary. Normal. Normal
Infraaxillary. Mid inspiratory crepts heard. normal(left)
Suprascapular normal normal
Interscapular normal normal
Infrascapular mid inspiratory coarse crepts (right and left)
Vocal resonance -normal over all areas
Cvs - s1,s2 normally heard ,no murmur
Jvp not raised
Cns-consious orientation ,no focal neurological deficit
PA- soft ,non tender,no organomegaly,normal bowel sound heard
Diagnosis
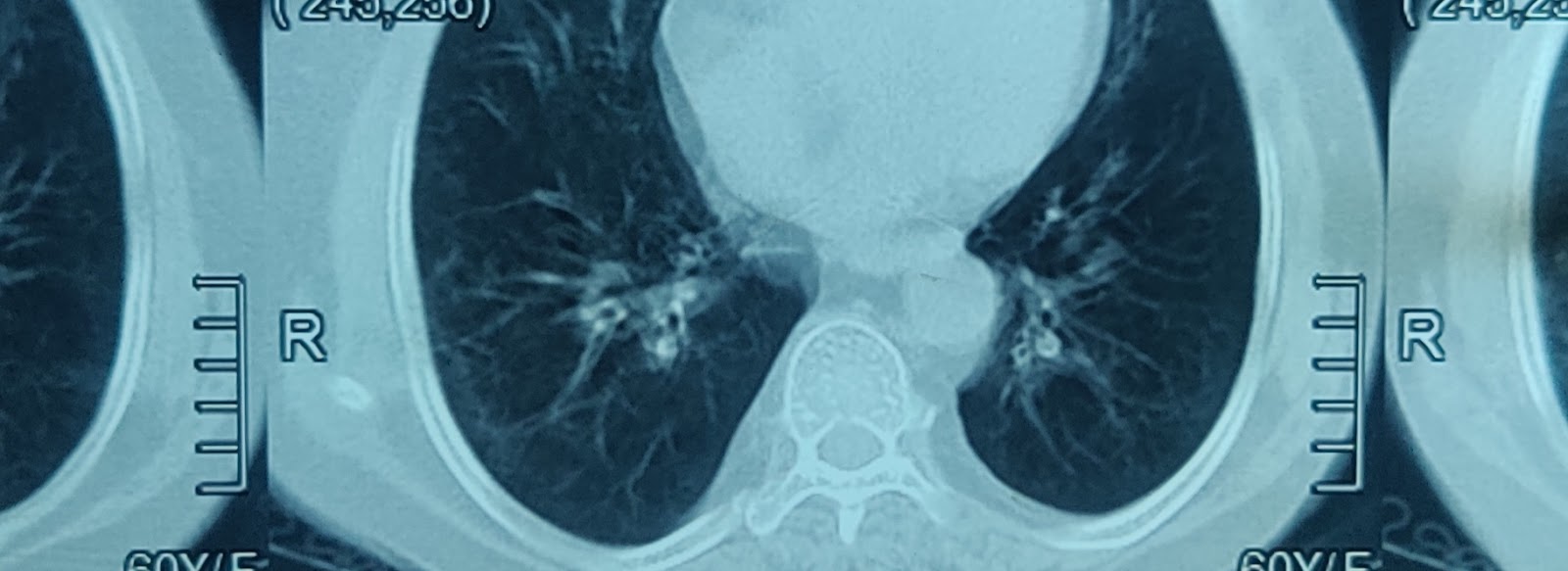
Right sided bronchiectasis associated with diabetic melitus
Investigation:
CBP-
Hb-11.7 gm/dl
Total leucocytosis-16,200cells/cumm
Platelet count- 3.98lakhs/cu.mm
Smear-normocytic normochromic with leucocytosis
Glycated hb-hbA1c -7%
Urine for ketone bodies absent
Complete urine examination -normal
Serum creatinine level-normal
Serum electrolyte level -normal
Liver function test -slight rise in alkaline phosphate level
C reactive protein -postive on 9/3/23
Negative -11/03/23
HBsag -negative
Hiv -negative
Chest x ray


Treatment:
Inj.augmentin 1.2gm iv tid
Inj.pantop 40mg iv od
T.Pcm 650mg po
Syp.Ascoril po tid 2tsp

T.glimipride 1mg +metformin 500mg bd
Syp.citralka 10ml in 1glass of water bd
Normal saline compressor
T.MVT
T.shelcal 500mg po od
Chest physiotherapy
Neb with mucomist 8th hrly &ipravent 6th hrly
O2 inhalation if spo2<94%
Good nutrition food


Comments
Post a Comment